Etiopathogenesis of Type 1 Diabetes
Type 1 diabetes (T1D) is a progressive, autoimmune disease resulting from CD4+ and CD8+ T cell-mediated destruction of pancreatic β cells; inflammatory infiltrate of pancreatic islets, or insulitis; genetic susceptibility associated with the human leukocyte antigen (HLA) region; and the development of autoantibodies reactive against β-cell antigens.1
Activated B cells interact with CD4+ and CD8+ T cells, and antigen presentation by B cells and dendritic cells drives the activation of cytotoxic, β-cell-specific T cells, also leading to the development of islet autoantibodies (IAbs) by B cells.2 The IAbs that target insulin, 65 kDa glutamic acid decarboxylase, insulinoma-associated protein 2, and zinc transporter 8—are associated with secretory granules in β cells. They serve as biomarkers of T1D-associated autoimmunity that are found months to years before symptom onset and can be used to identify and study individuals who are at risk of developing the disease.2 The figure below depicts the pathogenesis of T1D.

Other potential contributors to the disease include perinatal factors such as a lack of passive transfer of immune protection or embryonic insult, immunization timing, the use of cow’s milk formula, gut biome changes, and other environmental factors, including enteroviruses.1
Genetic susceptibility is confirmed in twin and immediate-family studies, with a 30% to 70% concordance of diagnosis in identical twins. There is a 6% to 7% increased risk of co-occurrence among siblings of an individual with T1D, as well as a 1% to 9% risk in children with a parent who has T1D (see Risk of Type 1 Diabetes table).3–6
Genetic susceptibility is mediated by polygenic features in HLA class II genes, which account for 40% to 50% of familial risk. The most frequent or high-risk alleles (present in up to 90% of patients with T1D) are HLA-DR3-Q2 and DR4-Q8.7 In addition, the presence of HLA‑DR and HLA‑DQ genotypes (HLA-DR-DQ) convey an increased risk of developing 2 or more autoantibodies and T1D.2
Individuals with T1D are also more likely to have other autoimmune disorders as well as monogenic polyglandular autoimmune syndromes.8

However, 90% of people diagnosed with T1D have no family history of the disease.10 This highlights the need for population-based screening.
Increasing Incidence and Prevalence of Type 1 Diabetes
An estimated 1.8 million adults in the United States and approximately 314,000 children and adolescents (<20 years old) have T1D. It is the most common form of diabetes in childhood and adolescence, but it can occur at any age. The incidence is increasing across age groups, including in adults, as shown in figures below, with an estimated 5 million people in the United States diagnosed with T1D by 2050, including nearly 600,00 children and adolescents.11 The first figure below depicts trends in the incidence of T1D in children and adolescents between 2002 and 2018; the second figure below highlights the incidence by age and sex between 2001 and 2015.


One study found a 1.9% annual percentage change in incidence from 2002 through 2015.13 Although the incidence of T1D is still high in non-Hispanic Whites, it is increasing at a faster rate in other racial and ethnic groups. Non-Hispanic Asian or Pacific Islander children and adolescents had the largest significant increases, followed by Hispanic and non-Hispanic Black children and adolescents.11
It is estimated that up to 40% of adults older than age 30 years with T1D may have been misdiagnosed with type 2 diabetes (T2D) or monogenic diabetes, with an increased risk for error associated with increasing age.14 Key challenges to a timely, accurate diagnosis in adults include the assumption that T1D is a disease of childhood and adolescents and that adults with diabetes have T2D. Yet up to 70% of all cases of T1D are adult-onset.15 This results in delayed diagnosis, worse symptoms, and delayed treatment.16–18
A survey of 3030 adults with T1D and parents of children with T1D found that 1 in 4 were misdiagnosed, resulting in an 18% increased risk for diabetic ketoacidosis (DKA) compared with those individuals with a correct diagnosis.17
Impact of Type 1 Diabetes on Quality of Life
Despite technological advances in the management of T1D, including continuous glucose monitoring and insulin pumps, hypoglycemia, hyperglycemia, and DKA are still common occurrences. They all have a significant impact on patient quality of life as well as long-term outcomes, including an increased risk of macro- and microvascular complications.19 Indeed, DKA is 1 of the most common causes of death in children with T1D, given the resulting cerebral edema.20
Adults may also present with DKA at diagnosis and after, although the frequency is unknown. However, the primary risk factor for adults is not undiagnosed T1D; the main risk factors are nonadherence with insulin use and infections.16
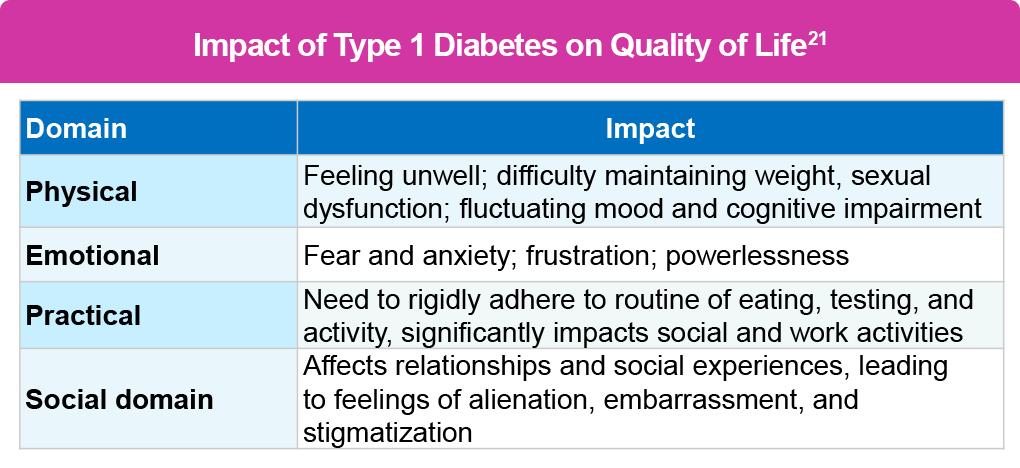
A review of 31 studies found that uncontrolled T1D—both immediate hypoglycemic episodes and longer-term hyperglycemia complications—adversely affects the physical, emotional, practical, and social domains of a patient’s life (see table below). The quality of life for the patients’ family members is also negatively impacted.21
References
- Atkinson MA, Mirmira RG. The pathogenic “symphony” in type 1 diabetes: a disorder of the immune system, β cells, and exocrine pancreas. Cell Metab. 2023;35:1500-1518.
- Katsarou A, Gudbjörnsdottir S, Rawshani A, et al. Type 1 diabetes mellitus. Nat Rev Dis Primers. 2017;3:17016.
- DiMeglio LA, Evans-Molina C, Oram RA. Type 1 diabetes. Lancet. 2018;391:2449-2462.
- Noble JA. Immunogenetics of type 1 diabetes: a comprehensive review. J Autoimmun. 2015;64:101-112.
- Pociot F, Lernmark Å. Genetic risk factors for type 1 diabetes. Lancet. 2016;387:2331-2339.
- Redondo MJ, Jeffrey J, Fain PR, et al. Concordance for islet autoimmunity among monozygotic twins. N Engl J Med. 2008;359:2849-2850.
- Noble JA, Valdes AM. Genetics of the HLA region in the prediction of type 1 diabetes. Curr Diab Rep. 2011;11:533-542.
- American Diabetes Association Professional Practice Committee for Diabetes. 2. Diagnosis and classification of diabetes: standards of care in diabetes – 2026. Diabetes Care. 2026;49(suppl 1): S27-S49.
- Parkkola A, Härkönen T, Ryhänen SJ, et al. Extended family history of type 1 diabetes and phenotype and genotype of newly diagnosed children. Diabetes Care. 2013;36:348-354.
- Sims EK, Besser REJ, Dayan C, et al. Screening for type 1 diabetes in the general population: a status report and perspective. Diabetes. 2022;71:610-623.
- Centers for Disease Control and Prevention. National Diabetes Statistics Report. https://www.cdc.gov/diabetes/php/data-research/index.html.
- Rogers MAM, Kim C, Banerjee T, Lee JM. Fluctuations in the incidence of type 1 diabetes in the United States from 2001 to 2015: a longitudinal study. BMC Med. 2017;15:199.
- Divers J, Mayer-Davis EJ, Lawrence JM, et al. Trends in incidence of type 1 and type 2 diabetes among youths—selected counties and Indian reservations, United States, 2002–2015. Morb Mortal Wkly Rep. 2020;69:161-165.
- The Lancet Regional Health-Europe. Misdiagnosis of type 1 and type 2 diabetes in adults. Lancet Reg Health Eur. 2023;29:100661.
- Burahmah J, Zheng D, Leslie RD. Adult-onset type 1 diabetes: a changing perspective. Eur J Intern Med. 2022;104:7-12.
- Leslie RD, Evans-Molina C, Freund-Brown J, et al. Adult-onset type 1 diabetes: current understanding and challenges. Diabetes Care. 2021;44:2449-2456.
- Muñoz C, Floreen A, Garey C, et al. Misdiagnosis and diabetic ketoacidosis at diagnosis of type 1 diabetes: patient and caregiver perspectives. Clin Diabetes. 2019;37:276-281.
- Thomas NJ, Lynam AL, Hill AV, et al. Type 1 diabetes defined by severe insulin deficiency occurs after 30 years of age and is commonly treated as type 2 diabetes. Diabetologia. 2019;62:1167-1172.
- Al Hayek AA, Al Dawish MA. Frequency of diabetic ketoacidosis in patients with type 1 diabetes using FreeStyle Libre: a retrospective chart review. Adv Ther. 2021;38:3314-3324.
- Wolfsdorf JI, Allgrove J, Craig ME, et al. ISPAD Clinical Practice Consensus Guidelines 2014. Diabetic ketoacidosis and hyperglycemic hyperosmolar state. Pediatr Diabetes. 2014;15(suppl 20):154-179.
- Vanstone M, Rewegan A, Brundisini F, et al. Patient perspectives on quality of life with uncontrolled type 1 diabetes mellitus: a systematic review and qualitative meta-synthesis. Ont Health Technol Assess Ser. 2015;15:1-29.