Importance of Early Detection of Type 1 Diabetes
Until recently, most people with T1D were diagnosed when they started showing symptoms of the disease. That has changed, with screening now recommended for anyone with a family history of T1D. Population-wide screening is likely to become the norm over the next few years. Such screening can detect the disease before symptoms develop, making early treatment possible.1
Anyone can get tested. But if you or your family have any relatives with T1D, they should definitely be tested since they already have a higher risk of the disease. In fact, if you have a first-degree family member (parent, child, or sibling) with T1D, you are 15 times more likely to develop T1D than someone without this connection.2
All it takes is a simple blood test, one you can do in your doctor’s office or even at home. The test measures levels of proteins called islet autoantibodies, markers that confirm your immune system is attacking and killing insulin-producing beta cells.1
There are 4 main islet autoantibodies that are typically used for screening, although others have been described.3 If you have 2 or more of these autoantibodies, you have a near 100% risk of developing T1D over your lifetime.3 In fact, screening for these autoantibodies in children at 2 years and between 5 and 7 years predicts most cases of T1D that will develop by the time the child is 15 years of age.4
Screening can also tell you what stage of T1D you have: stage 1, stage 2, or stage 3.5 Stages 1 and 2 do not have symptoms, but blood sugar levels become slightly elevated at stage 2, and by stage 3 they are high enough to meet the diagnostic criteria for diabetes; this is also when most people show symptoms.5 Stage 4 is long-standing T1D. As time goes on, the body’s ability to make insulin decreases.
See the figure below.
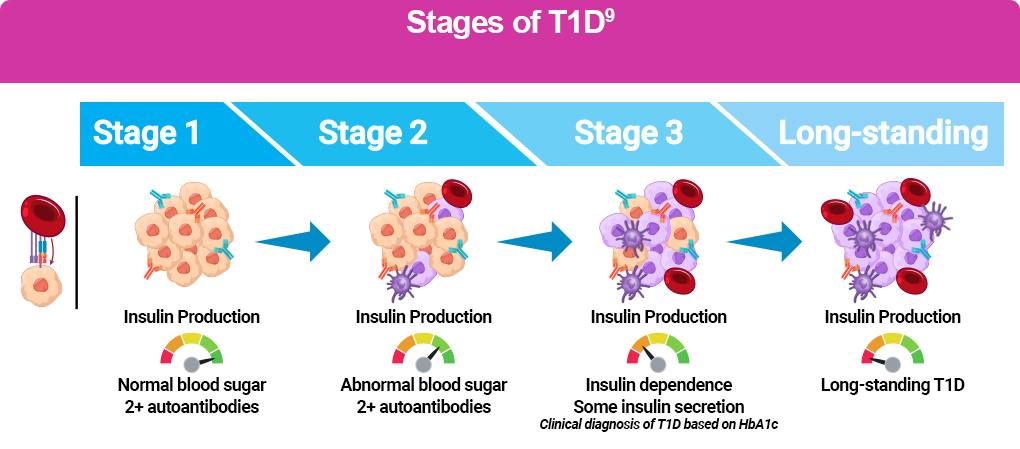
About 4 in 10 children with a genetic risk of T1D who are in stage 1 will develop T1D within 5 years, 7 out of 10 within 10 years, and 100% at some point in their lifetime. By stage 2, about 7 out of 10 will develop T1D within 5 years and 100% at some point in their lifetime.3,6
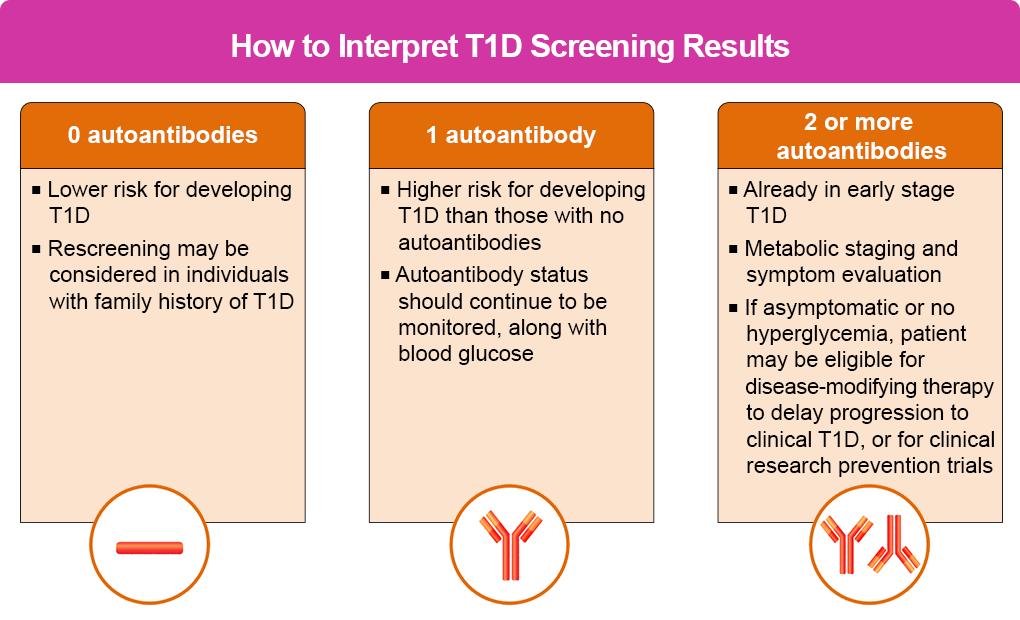
The figure below provides more detail, including the type of follow-up needed.
Benefits of Screening
Screening has several benefits, including1:
- Significantly reducing the risk of DKA, which can have lifelong benefits; in fact, identifying T1D before any symptoms appear slashes the rate of DKA from as high as 60% to less than 5%.
- Reducing the risk of hospitalization
- Providing you with time to learn about managing T1D and build a healthcare team
- Enabling you to join a clinical study
- Affording you the opportunity to receive the first US Food and Drug Administration (FDA)-approved drug shown to slow progression of stage 2 diabetes to clinical T1D
If you screen positive for even 1 autoantibody, your doctor will want to continue screening and testing your blood sugar levels every year. If you have stage 2 diabetes, your doctor will want to follow you more closely, possibly having you test your blood sugar at home as well as in the office. Even when your test is negative, if you have a high risk of T1D based on your family history, your doctor may want to screen you again later.7
Screening Programs
Several screening programs are available at the local and national levels. TrialNet is a national registry that provides in-home test kits and reports results in patient-friendly language, highlighting what the results mean.8 Your doctor may also be able to offer the test in their office or provide a referral to get tested through certain laboratories in your area.
TrialNet
This research-based screening and clinical trial program is available for those people who have a higher risk of developing T1D based on family history or previous autoantibody testing. Eligible individuals include:
- People between 2.5 and 45 years old who have a first-degree relative with T1D
- People between 2.5 and 20 years old who have a second-degree relative with T1D
- People between 2.5 and 45 years old who have tested positive for 1 or more T1D-related autoantibody outside of TrialNet
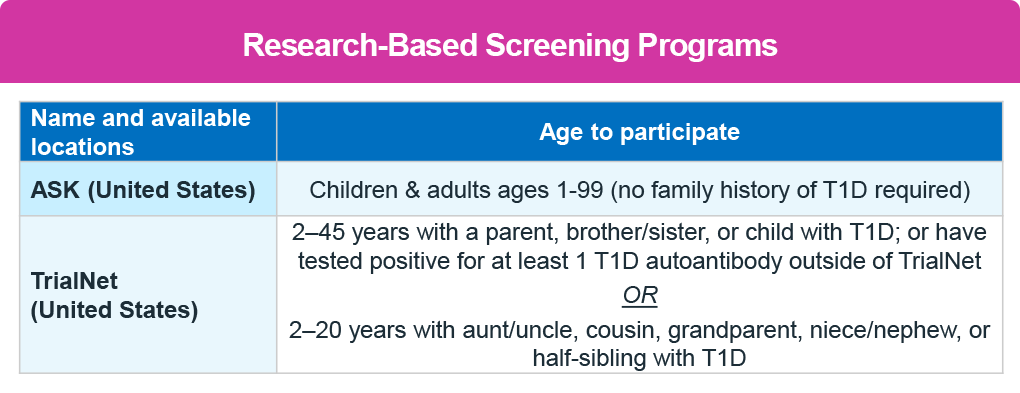
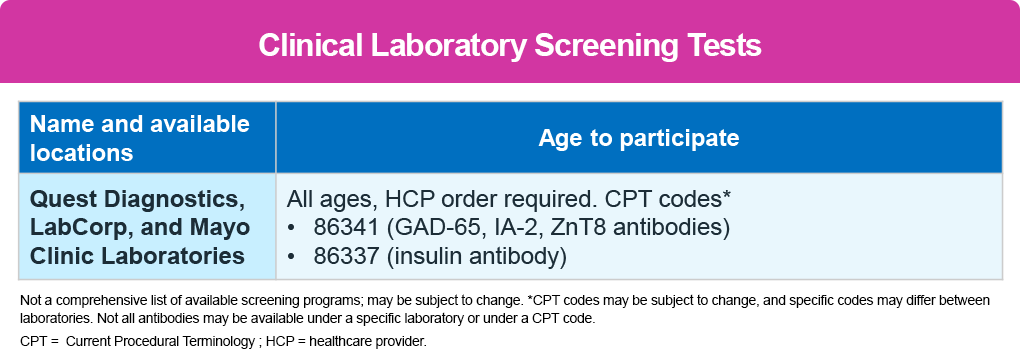
In addition, several other local screening programs are available as shown in the table below9, and more information can be found under the Resources section.
References
- Simmons KM, Sims EK. Screening and prevention of type 1 diabetes: where are we? J Clin Endocrinol Metab. 2023;108:3067-3079.
- Besser REJ, Bell KJ, Couper JJ, et al. ISPAD clinical practice consensus guidelines 2022: stages of type 1 diabetes in children and adolescents. Pediatr Diabetes. 2022:23:1175-1187.
- Ziegler AG, Rewers M, Simell O, et al. Seroconversion to multiple islet autoantibodies and risk of progression to diabetes in children. JAMA. 2013;309:2473-2479.
- Ghalwash M, Dunne JL, Lundgren M, et al. Two-age islet-autoantibody screening for childhood type 1 diabetes: a prospective cohort study. Lancet Diabetes Endocrinol. 2022;10:589-596.
- Greenbaum C, Lord S, VanBuecken D. Emerging concepts on disease-modifying therapies in type 1 diabetes. Curr Diab Rep. 2017;17:119.
- Insel RA, Dunne JL, Atkinson MA, et al. Staging presymptomatic type 1 diabetes: a scientific statement of JDRF, the Endocrine Society, and the American Diabetes Association. Diabetes Care. 2015;38:1964-1974.
- Mahon JL, Sosenko JM, Rafkin-Mervis L, et al. The TrialNet Natural History Study of the development of type 1 diabetes: objectives, design, and initial results. Pediatr Diabetes. 2009;10:97-104.
- TrialNet. Pathway to Prevention screening www.trialnet.org/our-research/risk-screening
- Breakthrough T1D (formerly JDRF). Information on early T1D detection. https://www.breakthrought1d.org/early-detection/