Clinical Presentation and Natural History of T1D
Type 1 diabetes (T1D) is a slowly progressive disease. It may take months or even years before symptoms severe enough for diagnosis develop, and by then patients are typically in a clinical crisis. However, multiple autoantibodies may be detected from a few weeks up to 20 years before the onset of clinical disease.1 Indeed, 90% of children who develop T1D before puberty have islet autoantibodies (IAbs) by 5 or 6 years of age, and many have IAbs by 2 years of age.2
The most common presentation of T1D in children is absolute insulin deficiency, leading to diabetic ketoacidosis (DKA), which has higher rates in African American and Hispanic children.3
The rate of β-cell destruction can vary significantly on both an individual level and across populations and age groups, with significantly faster progression at younger ages.1,6
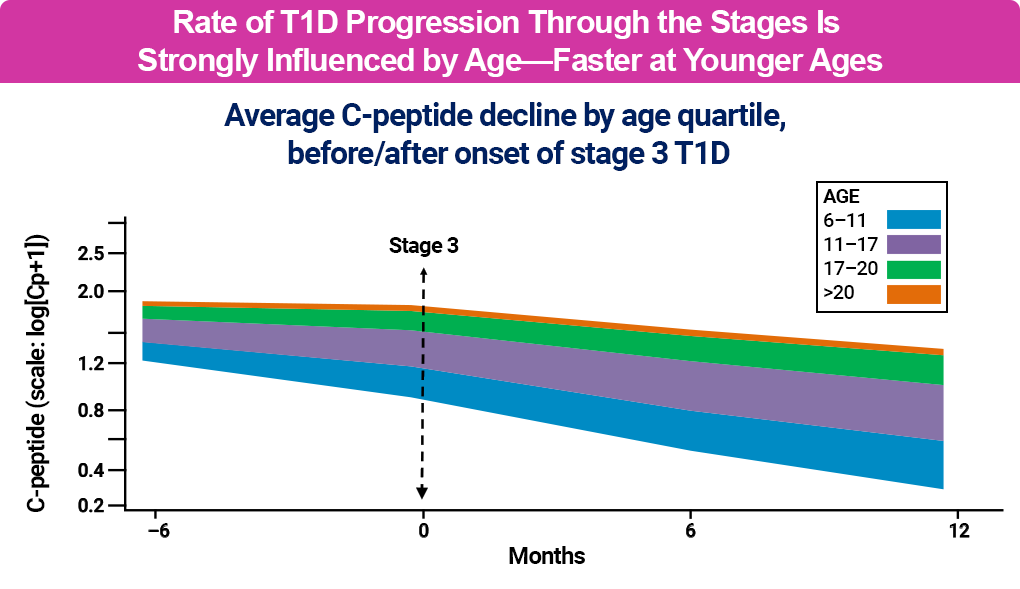
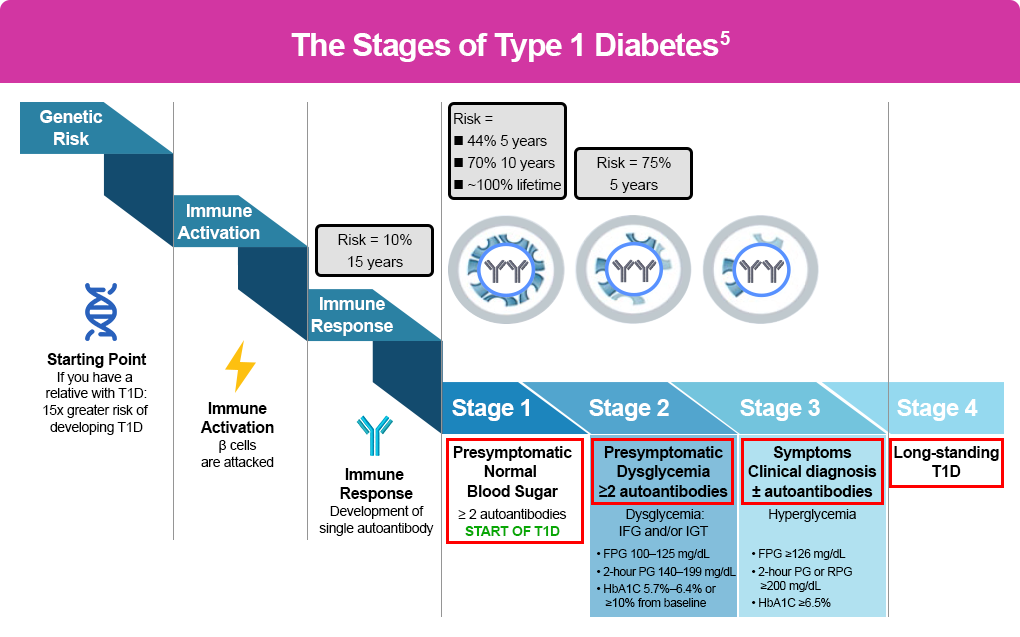
It also differs between individuals, with environmental, physiological, and genetic factors determining functional β-cell mass and C-peptide levels, a marker of endogenous insulin production.1,4 A model about T1D natural history, originally proposed in 1986, describes a somewhat linear concept of progression, from genetic predisposition to a progressive loss of insulin release and development of T1D, and is shown in black in the figure below.4 However, recent research suggests a heterogeneity of the natural history and progression of T1D, which is noted in blue in the figure below, and has improved our understanding of T1D progression and opportunities for asymptomatic screening, early detection, and early treatment.4

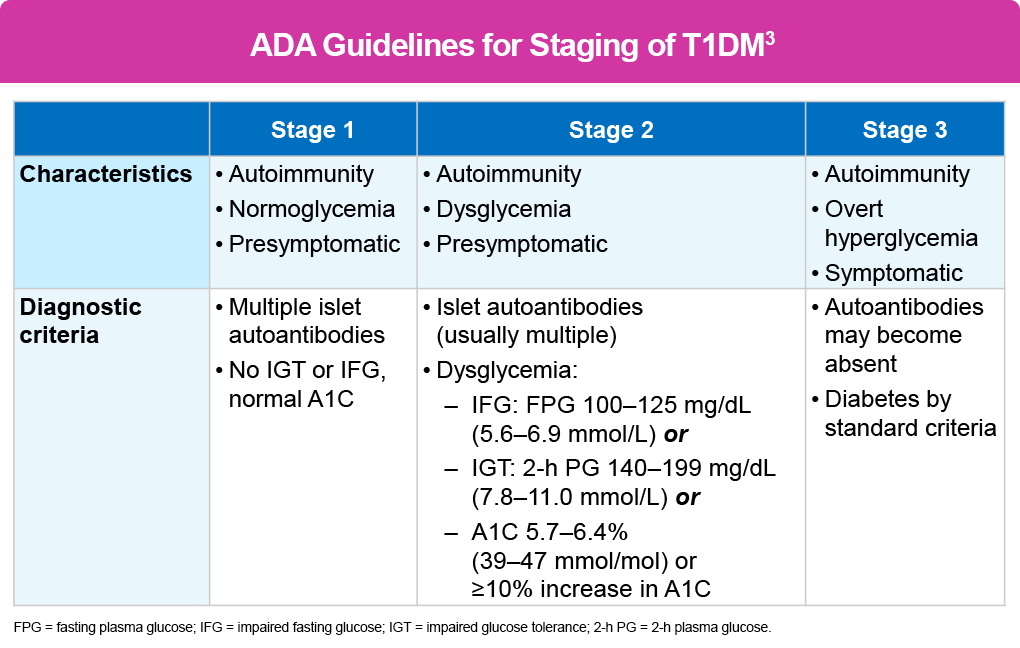
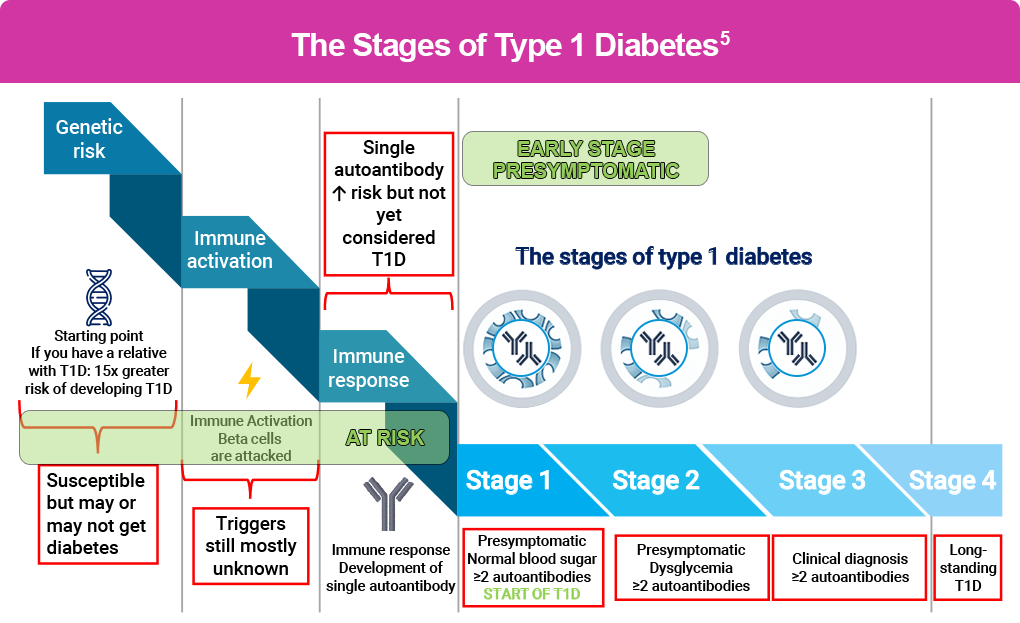
Based on the understanding of T1D progression and on the idea that once an individual develops more than 1 islet autoantibody, they have a near 100% lifetime risk of clinical disease, T1D is classified into stages related to risk.4,5 All stages are characterized by the presence of multiple islet autoantibodies (≥2), although antibodies may become absent in stage 3, and differ in symptoms and glycemic status, as shown below.4 Stages 1 and 2 are presymptomatic (also typically called early-stage T1D), with normoglycemia in stage 1 and dysglycemia in stage 2. Stage 3 is marked by the onset of symptoms, and diabetes is diagnosed by standard criteria. Stage 4 denotes long-standing T1D.
An individual with 1 positive islet autoantibody is considered at risk and has a 10% chance over 15 years of developing stage 3 T1D. In patients with stage 1 and stage 2 T1D, the risk of progressing to stage 3 is higher (as outlined in the figure below), with a near 100% lifetime risk once they develop 2 or more islet autoantibodies.1-7
References
- Ilonen J, Lempainen J, Veijola R. The heterogeneous pathogenesis of type 1 diabetes mellitus. Nat Rev Endocrinol. 2019;15:635-650.
- Ziegler A-G. The countdown to type 1 diabetes: when, how and why does the clock start? Diabetologia. 2023;66:1169-1178.
- American Diabetes Association Professional Practice Committee for Diabetes. 2. Diagnosis and classification of diabetes: standards of care in diabetes – Diabetes Care. 2026;49(suppl 1):S27-S49.
- Atkinson MA, Eisenbarth GS, Michels AW. Type 1 diabetes. Lancet. 2014;383:69-82.
- Haller MJ, Bell KJ, Besser REJ, et al. ISPAD clinical practice consensus guidelines 2024: screening, staging, and strategies to preserve beta-cell function in children and adolescents with type 1 diabetes. Horm Res Paediatr. 2024;97:529-545.
- Greenbaum CJ, Bean CA, Boulware D, et al. Fall in C-peptide during first 2 years from diagnosis: evidence of at least two distinct phases from composite Type 1 Diabetes TrialNet data. Diabetes. 2012;61(8):2066-2073.
- Sims EK, Besser REJ, Dayan C, et al. Screening for type 1 diabetes in the general population: a status report and perspective. Diabetes. 2022;71:610-623.